
By Megan Gunnar, Carrie DePasquale, and Melissa Engel
In our previous work, we found that the key stress system of the body learns about the world in the first year or so of life and sets itself to adapt to those conditions. If conditions are harsh and stressful, rather than remain reactive, it changes its regulation so that it does not produce high levels of cortisol, a powerful stress hormone. Remaining reactive might mean that, living in high stress conditions, it would frequently produce high levels of cortisol, which could be damaging to the developing brain and body. Opting to be hypo-reactive, though, also comes with its own problems. This is because part of the job of a cortisol stress response is to turn off and disrupt the activity of other stress-responsive systems like the immune system. When children grow up in safe and supportive environments, they can afford to have a reactive cortisol system, reaping the benefits of a stress response when it is needed.
Once set in infancy, can the cortisol stress system recalibrate if conditions change? We have seen that it stays set to a low level of reactivity for years after children reared in institution (orphanages) are adopted into supportive homes. Puberty, though, is a time the brain and body undergo marked changes. There is increasing evidence that during puberty the brain is more plastic, changeable and responsive to input from the environment. We wondered whether with puberty our stress system wakes up and “tests the waters” again, asking, in a sense, “how harsh and stressful will my adult life be?” If so, then it might be that the stress system of children adopted from harsh conditions in institutions would “recalibrate” and become more reactive, like that of children who were born into safe, secure, well-resourced conditions.
To answer this question we studied 321 children and adolescents (142 adopted, 179 non-adopted) over two full years. We had three assessment points: when participants first joined the study, then a year later and a year after that. At each assessment, nurses assessed the participants’ pubertal status, we had participants collect saliva for cortisol analysis at home on three days once upon waking up, then 30 minutes later, and at bedtime. Participants also took part in a social stress test that involved giving a speech and performing mental arithmetic aloud in front of judges while being videotaped. We also conducted an intensive interview from which we derived a measure of current life stress. We assessed the last participant in September of 2018. Since then we have been processing the tremendous amount of information these families and participants have provided. We have learned some very interesting things that we are delighted to share with you.

When children grow up in safe and supportive environments, they can afford to have a reactive cortisol system, reaping the benefits of a stress response when it is needed.
The Cortisol Stress Response Does Recalibrate
Last year we reported on the first full year of assessment during which the participants were between 7 and 15 years old. Comparing across age (as opposed to the same participant over time), we did see evidence that the stress system might be recalibrating. Nonetheless, because it wasn’t the same participants over time, we could not be truly sure that change was also taking place within each participant with puberty. Now that we have all three assessments, we are happy to report that the stress system does clearly appear to be “testing the waters” and resetting itself to the much more supportive conditions that the kids are now living in. It is as if the system is saying, “I can afford to be reactive, because my world is generally safe.”
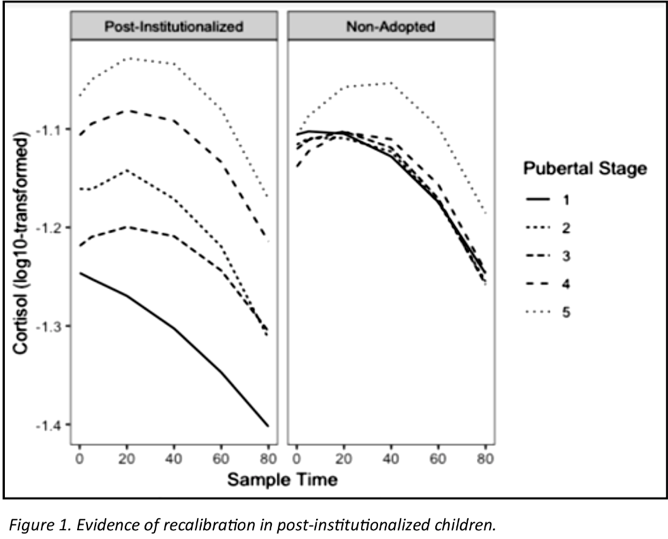
In the study, after the participants arrived in the research space we gave them some time to adapt to being with us and then began the stress test while repeatedly taking saliva samples for cortisol. During the test, participants spent 5 minutes preparing to give a speech about themselves, then they gave the speech for 5 minutes and afterwards did 5 minutes of mental arithmetic out loud all the while being judged and filmed and watching themselves in a mirror. The test was over in 15 minutes, but the cortisol stress system takes 25 minutes to reach peak levels, then it should start falling back to pretest levels. In Figure 1, the right panel shows data from the non-adopted kids. There really wasn’t much change in the cortisol response as a function of pubertal stage. The left panel shows data from the adopted kids. Stage one (lowest level and lowest cortisol) is before puberty really starts. You see that the adopted kids are not showing any cortisol response at all. By stages 2 and 3, however, we begin to see some response. By stages 4 and 5, the adopted youth cortisol response look very much like the non-adopted kids. This is the first clear demonstration that Dr. Gunnar’s pubertal stress recalibration hypothesis holds and it also is good news, we believe, for children adopted from orphanages.
Impact of early and current stress on the body’s alarm clock
It is hard to get up in the morning – so, our body has developed ways to help us. One aspect of the body’s physiological “alarm clock” is the cortisol awakening response (CAR). We also examined this response in the Puberty Study. Cortisol is commonly referred to as the “stress hormone”; however, it is also important for activating our metabolic and mental resources, and helps us maintain our circadian rhythm (a.k.a. our body’s internal clock).
The CAR helps us wake up in the morning by increasing cortisol production, particularly in the hour before and peaking 30-45 minutes after awakening. Some past research in our lab has shown that children adopted from orphanages show a less-pronounced (a.k.a. smaller increase) CAR compared to non-adopted children. However, we have suspected that puberty might be a window of opportunity during which aspects of cortisol regulation, including the CAR, could be “re-calibrated” to their current environment, which poses substantially fewer risks than the orphanage they experienced as an infant. For example, adopted children’s CAR might increase over time, to become comparable with non-adopted children’s CAR.
Last year we reported that the CAR was blunted for children and adolescents who were adopted from institutions if they were adopted later (after 16 months), but not if they were adopted earlier. That is, we saw no evidence of recalibration. This year we focused instead on examining change in the CAR from the first assessment to the second assessment. We did not find that this change differed for adopted and non-adopted children, thus so far we are really are not seeing evidence that it re-calibrates. What we have found is that both adopted and non-adopted children show a developmental change in the CAR that interacts with current life stress.
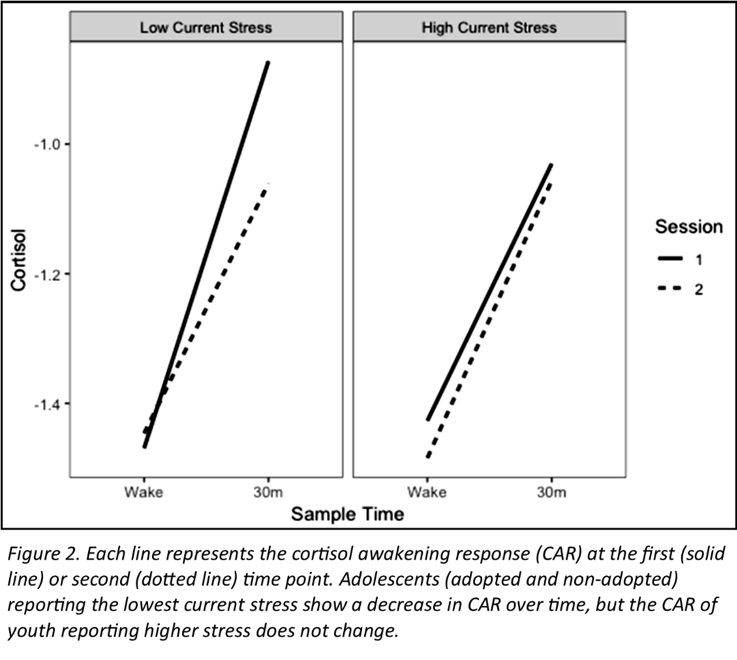
Previous studies, not in our research group, reported that the CAR increases as youth progress through puberty. In our study, with many more participants, we found that the CAR actually decreases as children progress through puberty, as seen in Figure 2. The decrease with development is seen especially for the youth whose lives are currently low in stressful experiences, but shows less of a decrease for those who currently experience higher life stress. That is, the kids who are currently reporting conflict with parents, problems in academics, and/or conflict with friends show less of the normative developmental decrease in the CAR seen in the other children.
Furthermore, a decreasing CAR from the first to the second assessment was predictive (statistically) of parents reporting less aggression and conduct problems. This supports the idea that, because cortisol functions as both a stress hormone and a part of our biological clock, moderate levels of cortisol (but not too high ortoo low) might be best for children’s development.
Stay tuned next year to see the full results looking at all three years of CAR and the change across puberty!
Other Findings from the Puberty Study: The Discordance Analysis
The Puberty Study provided us with such rich data that we were able to run additional analysis, including one that examined the extent to which parents and children agreed on their reports of the child’s anxiety and depressive symptoms. Anxiety and depression are internal states. Unless the child shares what they are feeling and thinking with the parent, the parent can only guess at how anxious or depressed the child is. This is why, especially as children become adolescents, psychologists rely increasingly on what the kids tell them about anxiety and depression. Nonetheless, discrepancies between parent and child reports of the child anxiety and depression suggest that the child isn’t using the parent to help regulate these emotions, or the parent isn’t understanding what the child is trying to convey. Either way, we might expect that child to report more stress in their lives because parent and child are not seeing the child in the same way.
For both post-institutionalized and non-adopted youth, the more the parent’s report differed from the child’s report, the more stress children described in their lives.
We examined data from the first two assessments of the Puberty Study. At each assessment, we asked parents and children to complete questionnaires rating children’s anxiety and depressive symptoms. We then looked at the absolute discrepancy between parent and child report measures. At each assessment, we also conducted a stress interview with the child.
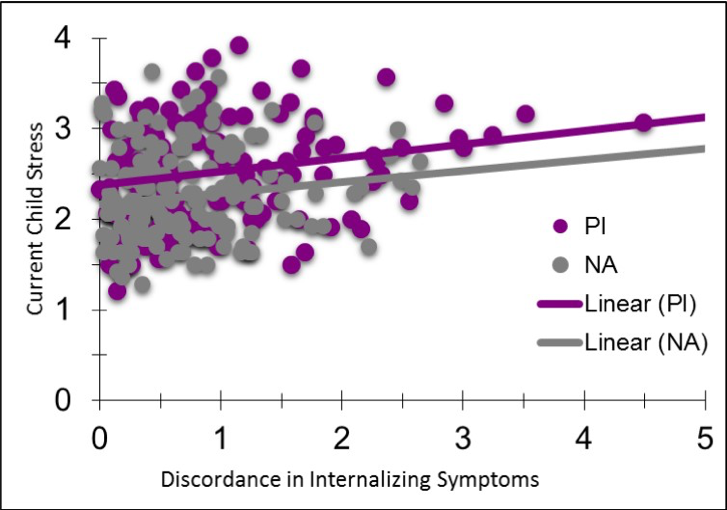
As we predicted, the more discrepant the parent and child reports on the child’s anxiety and depressive (i.e., internalizing) symptoms, the more stress the child described in their lives. This was true regardless of the child’s age and it was true for both of the years of assessments. Adopted (PI or previously institutionalized) kids and their parents were more discrepant in their reports on anxiety and depression, but for both adopted and comparison (non-adopted, NA) kids, the more the parent’s report differed from the child’s report, the more stress children described in their lives, as seen in Figure 3.


